This blog post is part of a series featuring new articles published in the LCNTDR Collection: Advances in scientific research for NTD control, led by the London Centre for Neglected Tropical Disease Research (LCNTDR). Stay tuned for updates on Twitter @bugbittentweets and @NTDResearch. You can find other posts in the series here.
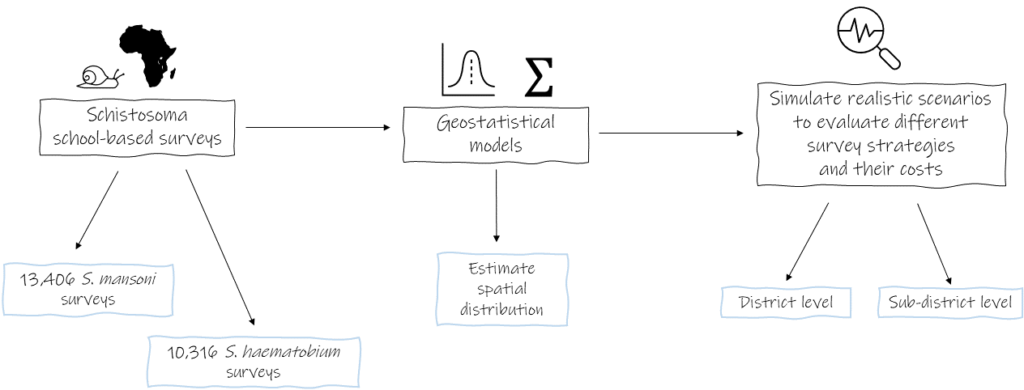
Schistosomiasis treatment programs use school-based surveys to determine where and how often treatment through mass drug administration should be carried out. However the spatial distribution of schistosomiasis is very focal, and affected areas may not be detected during surveys, leading to under treatment of affected communities. In our article we describe the use of geostatistical models to a) determine the spatial variations of the two main Schistosoma species affecting humans in sub-Saharan Africa, b) evaluate the accuracy of different survey designs to correctly identify treatment needs and c) determine the cost-effectiveness of different survey designs to guide schistosomiasis treatment programs.
Schistosomiasis
Schistosomiasis is a parasitic disease infecting over 150 million people in sub-Saharan Africa. Schistosoma parasites live in certain species of freshwater snails, with people often infected through contact with contaminated water sources. Due to this, there is substantial spatial variation in the burden of schistosomiasis, with communities living in close proximity to snail habitats or without access to clean water disproportionately affected. The main method of schistosomiasis control is mass drug administration preventatively treating school aged children within these communities. However, in order to determine which communities to treat, schistosomiasis control programmes first need to identify infection levels and targets for treatment. This becomes increasingly challenging after multiple rounds of mass drug administration, which can lead to an overall decrease in infection prevalence with isolated high burden areas remaining. Recent World Health Organization guidelines suggest classifying an implementation unit (typically a district or ecological zone) based on the mean prevalence of school-based surveys, with implementation units with a mean prevalence greater than 10% targeted for mass drug administration.
Geostatistical models for schistosomiasis
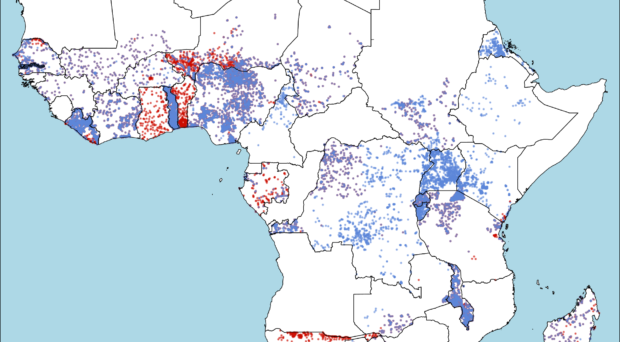
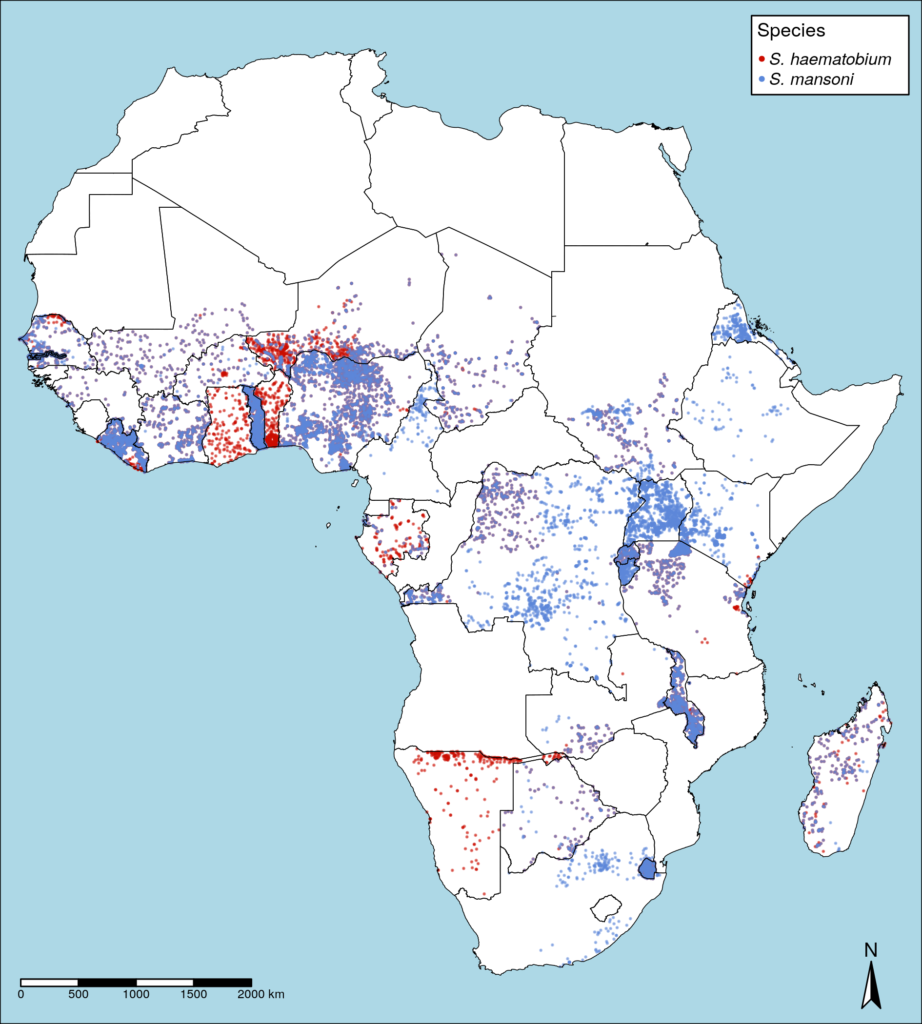
To examine the effects of survey design on the identification of areas for mass drug administration, we used simulations of the spatial distributions of Schistosoma haematobium and S. mansoni prevalence found across sub-Saharan Africa (infographic below).
We used geostatistical models to:
- Examine the spatial patterns of schistosomiasis across sub-Saharan Africa;
- Evaluate the accuracy of survey designs to determine areas for mass drug administration considering these spatial distributions; and
- Assess the cost of different survey designs.
We used data from 23,722 school-based surveys across sub-Saharan Africa. Using this data, we fit geostatistical models of spatial patterns of S. haematobium prevalence for 24 countries and S. mansoni for 28 countries (shown in the map of Africa below). Within this data, 29.5% (3039/10316) of schools reported a prevalence of S. haematobium of 10% or greater while 18.9% (2529/13406) of schools surveyed for S. mansoni reported over 10% prevalence. However, many districts with a mean prevalence below 10% which would be classified as not requiring treatment, still contained numerous schools with schistosomiasis prevalence above this threshold. Additionally, we identified substantial variations in the spatial patterns of schistosomiasis detected for different species in different countries.
The impact of survey design on schistosomiasis control programmes
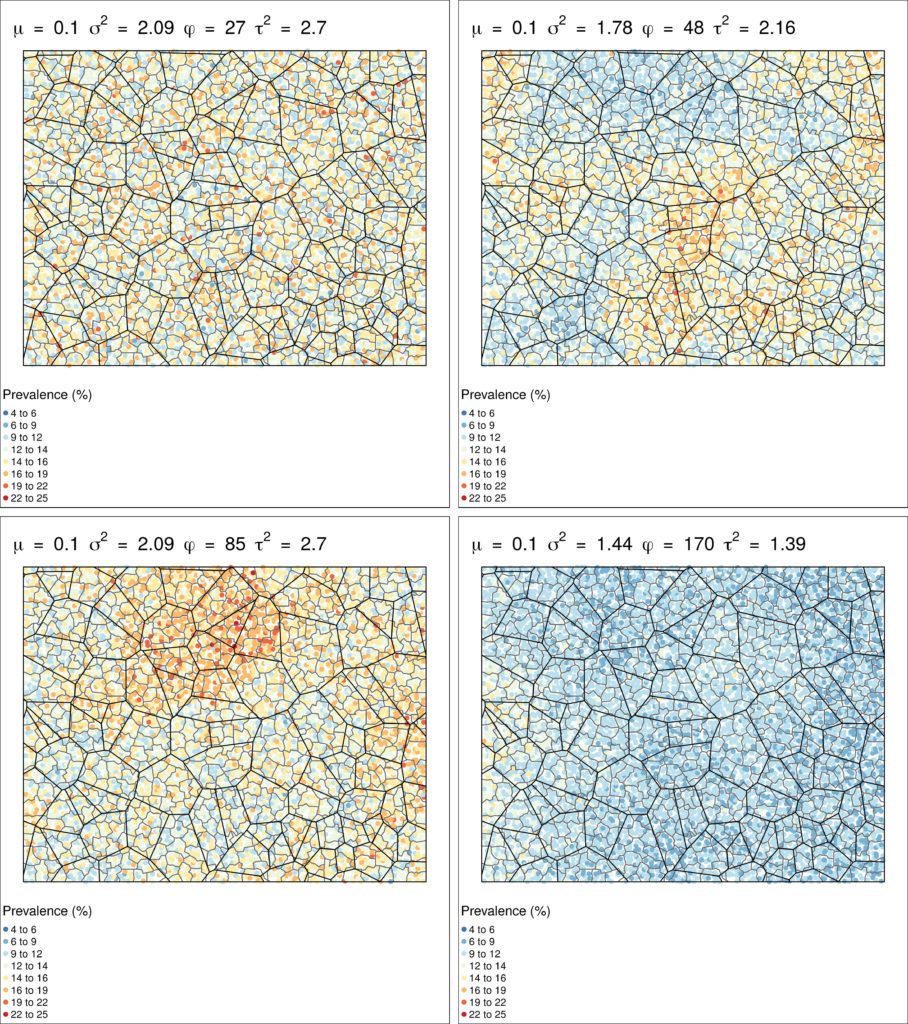
To examine the impact of survey design on classification of areas for treatment across all possible schistosomiasis distributions, we created a simulated hypothetical country the size of the mean area of all countries in sub-Saharan Africa with 15,000 total schools (a similar school density to Uganda). We divided this country into districts the median size of implementation units in sub-Saharan Africa, with each district comprising five subdistricts. We then used parameters from geostatistical models to simulate the range of possible schistosomiasis prevalence surfaces, generating 297 unique plausible scenarios, as shown in this figure.
Using these scenarios, we evaluated the accuracy and cost of three different survey methods:
- Randomly sampling five schools per district and assigning treatment to the district using mean prevalence (current strategy);
- Randomly sampling five schools per subdistrict and assigning treatment at subdistrict levels;
- Randomly sampling one school per subdistrict and assigning treatment at subdistrict levels
Results illustrated that sampling five schools per subdistrict resulted in the highest accuracy, both in terms of correctly classifying the mean district level prevalence and in the number of schools assigned to the correct treatment category. However, this level of sampling was highly intensive and therefore the most expensive and least cost-effective method. Alternatively, sampling one school per subdistrict and assigning treatment at subdistrict level increased the accuracy of treatment classification and was the most cost-effective option.
Balancing cost and accuracy
This study illustrates the importance of considering spatial patterns of prevalence when designing surveys and highlights how using smaller implementation units may improve treatment classification accuracy. Control programmes need to weigh the increased accuracy of more detailed and intensive survey strategies against survey costs and treatment priorities.
![]() The study featured in this blog post has been just published in the LCNTDR Collection: Advances in scientific research for NTD control, led by the London Centre for Neglected Tropical Disease Research (LCNTDR). The collection has been publishing in Parasites & Vectors since 2016, and releasing new articles periodically. This series features recent advances in scientific research for NTDs executed by LCNTDR member institutions and their collaborators. It aims to highlight the wide range of work being undertaken by the LCNTDR towards achieving the United Nations Sustainable Development Goals as well as supporting the objectives of the World Health Organization road map for neglected tropical disease 2021-2030.
The study featured in this blog post has been just published in the LCNTDR Collection: Advances in scientific research for NTD control, led by the London Centre for Neglected Tropical Disease Research (LCNTDR). The collection has been publishing in Parasites & Vectors since 2016, and releasing new articles periodically. This series features recent advances in scientific research for NTDs executed by LCNTDR member institutions and their collaborators. It aims to highlight the wide range of work being undertaken by the LCNTDR towards achieving the United Nations Sustainable Development Goals as well as supporting the objectives of the World Health Organization road map for neglected tropical disease 2021-2030.
The LCNTDR was launched in 2013 with the aim of providing focused operational and research support for NTDs. LCNTDR, a joint initiative of the Natural History Museum, the London School of Hygiene & Tropical Medicine, the Royal Veterinary College, the Partnership for Child Development, the SCI Foundation (formerly known as the Schistosomiasis Control Initiative) and Imperial College London, undertakes interdisciplinary research to build the evidence base around the design, implementation, monitoring and evaluation of NTD programmes.
You can find other posts in the series here.

{kind=link}
Comments