
Scabies
Scabies is a severe itchy skin disease caused by infection with the microscopic human itch mite Sarcoptes scabei var hominis. Scabies is found worldwide with over 400 million cases of scabies each year. Scabies is also one of the most common skin issues encountered by healthcare providers in low-income settings. In 2017, the World Health Organization recognized scabies as a Neglected Tropical Disease (NTD), leading to the development of scabies control programs.
Once a person is infected, the scabies mite burrows into the upper skin layer of the skin where it lives and lays its eggs. The most common symptoms of scabies are intense itching and a pimple-like skin rash. The itching and rash each may affect most of the body or be localized to areas such as the wrist, elbow, armpit, webbing between the fingers, nipple, penis, waist, belt-line and buttocks. The scabies mite is typically spread by direct, prolonged, skin-to-skin contact with an infected person.
Diagnosis of scabies involves a thorough patient history and detailed clinical examination. In many low-income settings, there is a lack of trained individuals with skin disease expertise and non-expert examiners are expected to see these patients. While promising strategies have been developed to help non-expert examiners diagnose scabies, a challenge has been the lack of validated diagnostic criteria for scabies.
To progress this, the International Alliance for the Control of Scabies (IACS) recently developed a detailed description of diagnostic criteria for three levels of diagnostic certainty:
- A – Confirmed Scabies, requiring visualization of the mite, eggs (ova) or fecal matter (scybala)
- B – Clinical Scabies
- C – Suspected Scabies
A prospective study was subsequently conducted to provide a detailed description of the morphology and distribution of scabies lesions (papules, vesicles, nodules and burrows) as assessed by dermatologists, and to validate the IACS Criteria for diagnosis by both expert and non-expert examiners.
The Validation Study
This diagnostic accuracy study took place in Monrovia, Liberia in February 2020. Participants (adults and children) were assessed independently by two dermatologists and six non-expert examiners who were trained over 2 days prior to the validation study. Skin lesion morphology and distribution were recorded based on the dermatologist examination. Diagnoses were classified by the IACS Criteria and the sensitivity and specificity of non-expert examiner assessments relative to the consensus diagnosis of the two experts was calculated.
Utility of the IACS Criteria in community settings
The expert and non-expert examiners each evaluated 135 individuals. The expert examiners also examined an additional 12 participants who were excluded from sensitivity and specificity calculations.
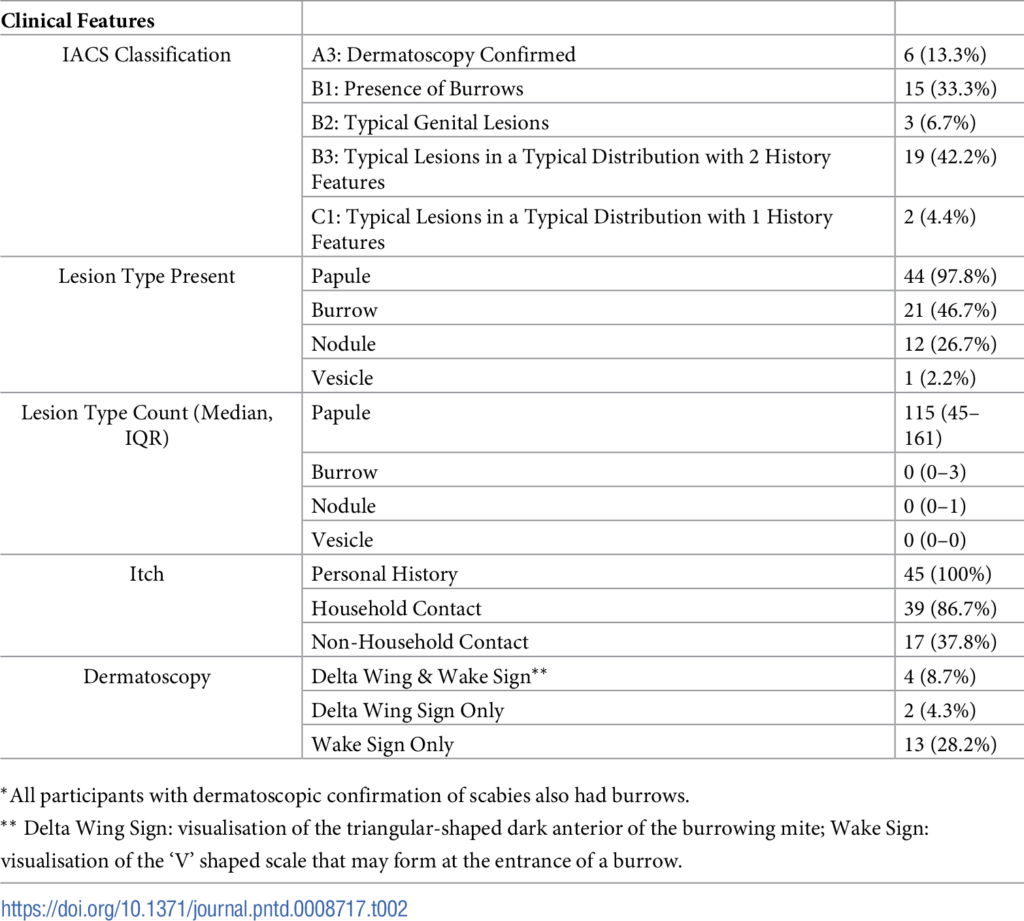
Among the total 142 individuals evaluated by the dermatologists, scabies was the most common skin diagnosis (29.9%). Forty-five individuals diagnosed with scabies underwent a comprehensive examination including full body examination, lesion counting and dermatoscopy.
Papules were the most common lesions (97.8%), while burrows were found in nearly half of infected participants (46.7%). All individuals with scabies reported a personal history of itch and 43 (93.5%) reported a history of contact with an individual with itch. The dermatoscopy was positive in only a minority of infected individuals (13.3%), showing limited sensitivity for scabies detection. Although scabies lesions were found in all body regions, the dermatologists found that over 90% of patients could have simply been diagnosed by examining only the limbs. The number of lesions present was also significantly associated with severity of patient reported itch (p = 0.003).
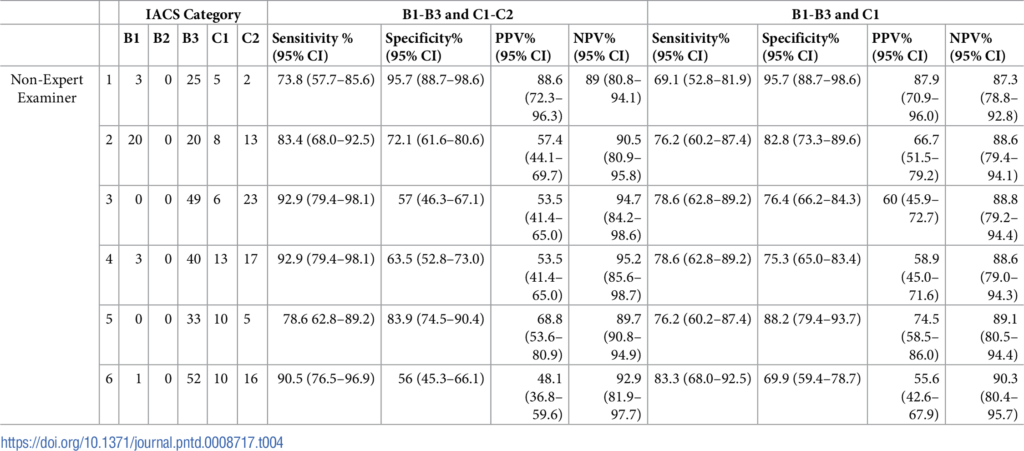
When IACS Categories B1, B3 and C1 (diagnostic of typical lesions or typical distribution pattern) were examined, the ability of non-expert examiners to detect typical scabies had a sensitivity ranging between 69–83% and a specificity between 70–96%. In non-expert examiners, the sensitivity was lower in infected individuals with fewer lesions (range 30-60%) and higher in more extensive disease (78–94%). During examinations, 160 false positive diagnoses were made by the non-expert examiners, of which 104 of 160 (65%) were accounted for by other skin conditions (such as atopic dermatitis/eczema, folliculitis, tinea corporis and capitis, lichen simplex, lichen planus and pityriasis versicolor).
Conclusions
This is the first study to undertake validation of the 2020 IACS Consensus Criteria for the Diagnosis of Scabies. The authors of the current study found that agreement between the two expert examiners on the presence of scabies was high (96% of cases), providing confidence in the reference standard diagnosis. The high level of diagnostic accuracy achieved by the non-expert examiners in this study indicates that this cadre of health professional is an effective resource for the diagnosis of scabies in LMICs. The IACS Criteria therefore was shown to be a valid tool for scabies diagnosis. Further studies are needed to evaluate the validity and reliability of the IACS Criteria in other settings, rural and urban, community-based, and in healthcare facilities with other cadres of workers.

Comments