
This blog post is part of a series featuring new articles published in the LCNTDR Collection: Advances in scientific research for NTD control, led by the London Centre for Neglected Tropical Disease Research (LCNTDR). Stay tuned for updates on Twitter @bugbittentweets and @NTDResearch. You can find other posts in the series here.
Schistosomiasis
Schistosomiasis is caused by parasitic worms that live in freshwater. It is also known as Bilharzia (after Theodor Bilharz who first discovered the adult worms post mortem), snail fever (the intermediate host are freshwater snails), or swimmer’s itch (due to the rash caused where the worms enter the skin). Schistosomiasis is the second most prevalent tropical disease in Africa after malaria. Although it does not kill to the extent of malaria, schistosomiasis can lead to complications such as chronic fatigue, anemia, physical and cognitive stunting, organ damage and fatal conditions, such as bladder cancer and increased susceptibility to HIV/AIDS.
It is difficult to know how many individuals die of schistosomiasis each year because death certificates seldom identify schistosomiasis as the primary cause of death. The prognosis is very good with early treatment, but people can die if it is left untreated. Unfortunately, schistosomiasis is often left undetected for several years. In fact, cyclist Chris Froome was not diagnosed until a blood test in 2010, the treatment of which may have helped his Tour de France win in 2013! The severity of the disease depends on the number of worms and how long the person has been infected.
Mass drug administration
Mass drug administration (MDA) is a strategy used to deliver medicine to the entire at-risk population of an area, most commonly a district. MDA with praziquantel is the main strategy for schistosomiasis control. In 2001, the World Health Organization (WHO) developed a “dose pole” for the administration of praziquantel, which estimates the optimal dosage according to an individual’s height. This invention has enormously facilitated the administration of the drug in large-scale interventions where whole communities are treated en masse by the local health worker.
School-based treatment or community-wide treatment
In Niger and most African settings, the control strategy is school-based treatment (SBT) with praziquantel, following the WHO guidelines. The rationale for this approach is that school-aged children harbor the burden of schistosomiasis infections due to their higher recreational water contact in rivers and ponds. There is a growing body of evidence regarding the burden of infection in adults and their potential role in sustaining transmission, which suggests a need for them to be included in treatment programs. There is debate around whether there is a cost-benefit to expanding treatment to community-wide treatment (CWT) and how to juggle this conundrum with a global shortage of praziquantel, which could not support countries worldwide scaling SBT up to CWT.
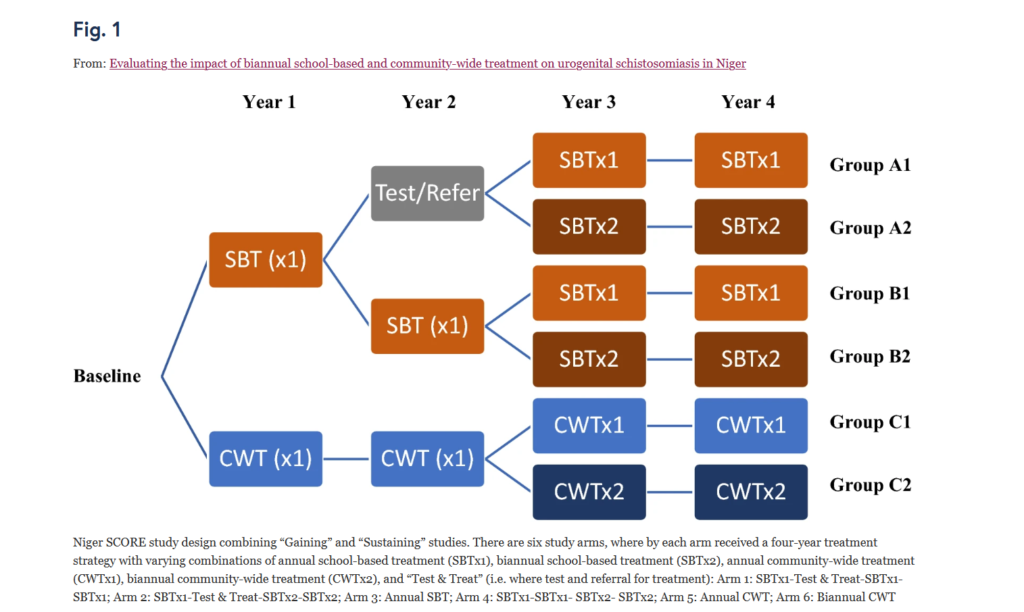
This study reviewed which treatment strategy provided the greatest reduction of schistosomiasis over five years comparing SBT once a year, SBT twice a year and SBT using test & treat (no MDA), CWT once a year and CTW twice a year (see figure).
This resulted in five major findings:
- Starting prevalence of infection will determine the strategy: In areas of high prevalence (i.e. a lot of infection in a community) treatment in schools twice a year was more impactful than treatment every year. In low prevalence settings there was no significant effect on treatment frequency.
- Adults benefit indirectly from treatment of school-aged children only: Adults tested in the annual SBT group also showed a decrease in schistosomiasis infection across the five years.
- Adults should be included in the monitoring and evaluation of schistosomiasis programs: These results show that monitoring and evaluation of school-aged children is not a successful indicator of the burden of infection in adults, and the justification for community wide treatment should include adults in evaluation surveys.
- Treatment alone is not sufficient to eliminate schistosomiasis: The lack of statistical impact of two rounds of treatment in low prevalence settings indicate that it may not be possible to break transmission through treatment alone and using other strategies, such as health education, water, sanitation and hygiene (WaSH) and snail control, should also be considered.
- Accuracy of coverage and compliance is challenging but the key to success: The success of schistosomiasis control is dependent on high treatment coverage and compliance. Average treatment coverage in this study was well above the WHO 75% threshold, in some areas above 100%, which is not uncommon for control programs to report. This highlights the need for control programs to be scrupulous in getting a reliable denominator. Furthermore, even when the proportion of the targeted population receiving treatment is high (coverage), those ingesting all the tablets (compliance) may be a better indicator of how well MDA is implemented.
These findings are an important consideration for schistosomiasis control programs that are considering elimination and support the idea that scaling up the frequency of treatment rounds, particularly in areas of low prevalence, will not eliminate schistosomiasis. The finding that prevalence in the community can be reduced, even where only school children are being treated, could have logistical and cost-saving implications for the national control programs.
![]() The study featured in this blog post has been just published in the LCNTDR Collection: Advances in scientific research for NTD control, led by the London Centre for Neglected Tropical Disease Research (LCNTDR). The collection has been publishing in Parasites & Vectors since 2016, and releasing new articles periodically. This series features recent advances in scientific research for NTDs executed by LCNTDR member institutions and their collaborators. It aims to highlight the wide range of work being undertaken by the LCNTDR towards achieving the United Nations Sustainable Development Goals as well as supporting the objectives of the World Health Organization road map for neglected tropical disease 2021-2030.
The study featured in this blog post has been just published in the LCNTDR Collection: Advances in scientific research for NTD control, led by the London Centre for Neglected Tropical Disease Research (LCNTDR). The collection has been publishing in Parasites & Vectors since 2016, and releasing new articles periodically. This series features recent advances in scientific research for NTDs executed by LCNTDR member institutions and their collaborators. It aims to highlight the wide range of work being undertaken by the LCNTDR towards achieving the United Nations Sustainable Development Goals as well as supporting the objectives of the World Health Organization road map for neglected tropical disease 2021-2030.
The LCNTDR was launched in 2013 with the aim of providing focused operational and research support for NTDs. LCNTDR, a joint initiative of the Natural History Museum, the London School of Hygiene & Tropical Medicine, the Royal Veterinary College, the Partnership for Child Development, the SCI Foundation (formerly known as the Schistosomiasis Control Initiative) and Imperial College London, undertakes interdisciplinary research to build the evidence base around the design, implementation, monitoring and evaluation of NTD programmes.
You can find other posts in the series here.

Comments