
Welcome to our SDG Editorial Board Members blog collection. We are hearing from the Editorial Board Members of the BMC Series journals whose work aligns with achieving the Sustainable Development Goals. Here you can find other posts in this collection, grouped with the tag ‘SDG editorial board members’.
Crises can either be transformative or disruptive. The COVID-19 pandemic has unfortunately exposed more of the latter as countries revert to nationalistic tendencies that intensify health inequities. Monitoring from UNDP data has shown that 1 in 2 people in high-income countries (HICs) have received a shot of the COVID-19 vaccine, while only 1 in 30 have received the same in low-income countries.
Whether between or within countries, health inequity is a major issue requiring global cooperation and strong health systems. The launch of the Sustainable Development Goals (SDGs) in 2015 provided an opportunity to demonstrate that global cooperation is possible.
Our research and policy work centers on SDG 3, the goal that seeks to ensure healthy lives and wellbeing for all. Our research values the idea that a robust ecosystem of Health Policy and Systems Research (HPSR) will contribute to getting countries back on track towards SDG 3 despite the challenges of COVID-19.
In this blog, we showcase an example of our SDG-related work and discuss our reflections from our participation in a convening series from May to June 2021. Around 50 representatives of HPSR institutions across Asia gathered virtually to co-create a vision and action plan for a robust HPSR ecosystem for the region. Asia is a region that has witnessed the emergence of an HPSR landscape that is diverse yet with shared challenges and opportunities. Results for Development and the WHO Alliance for HPSR led the co-creation process with support from USAID and the Bill & Melinda Gates Foundation.
From Push towards Co-creation
The challenge in using evidence for decision-making was a frequent HPSR issue that emerged in our discussions. The traditional model of evidence translation suggests two worlds: researchers who generate evidence and policymakers who use that evidence. Current approaches based on push models view evidence generation and policymaking as separate processes, where the evidence is pushed for use in policy, as suggested by the phrase evidence-informed policymaking. There is, however, emerging consensus that push or one-way models may even aggravate tensions between researchers and policymakers. Researchers become siloed in research without contributing to policy, while policymakers become siloed in developing policies without drawing on evidence. A co-creation model of doing HPSR, similar to the experience shared by Dr. Gloria Nenita Velasco of the Philippine Department of Health, can break these siloes down. In this example, the government determines and funds the research agenda while also closely collaborating with HPSR institutions across all stages of the research cycle to address the agenda.
Moving away from push models towards co-creation can ensure broader and meaningful participation of stakeholders. Co-creation is the process of bringing people together to define a problem collectively, identify solutions, and build consensus around action. Drawing on the idea of co-creation, we developed through a series of virtual sessions the following overarching HPSR vision for Asia: “A stronger enabling HPSR ecosystem of the future that is highly responsive to countries’ needs.”
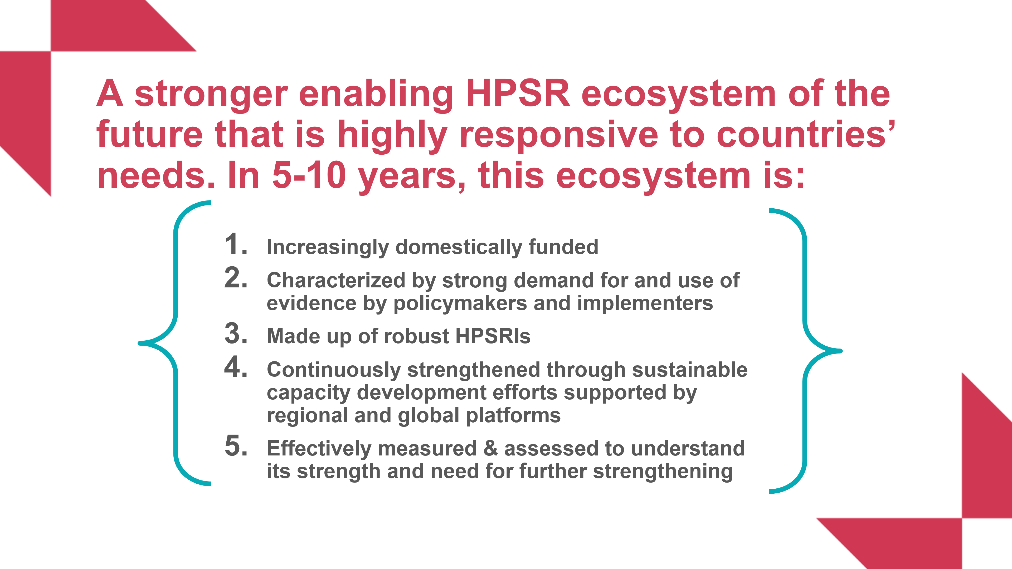
This co-created vision had five key components from which the participants also identified several pathways for success. A common feature of the various pathways was the idea of ensuring co-creation as well within the activities of the HPSR ecosystem. These pathways included secondments or exchanges between HPSR institutions and government agencies to collaborate on policy questions, as well as implementation research, capacity development, and research agenda-setting that bring together government and other stakeholders through networks or other co-creative mechanisms.
A robust HPSR ecosystem contributes to making health systems equitable, resilient in times of crisis, and more responsive to ensure people’s health and wellbeing. Co-creation can help secure buy-in, especially from stakeholders in LMICs who will be instrumental in realizing this vision of a robust HPSR ecosystem. For UNU-IIGH, this means building on existing collaboration with the Malaysian Ministry of Health and other partners in Asia to sustain HPSR capacity development in the region. Likewise, the vision compels HPSR institutions in the region to co-create the conditions that can set the stage for the effective use of evidence for policies in global health. As we aim for this vision, co-creation will require us to confront the power structures that maintain inequities in health policies and systems and ensure meaningful participation from LMICs and those with marginalized voices.
Co-creation needs Co-action
The enabling HPSR vision we have co-created for Asia, the global strategy to beat COVID-19, and the SDGs are all only lofty visions without implementation in practice. Co-action, the process of stakeholders united in moving together to translate their co-created ideas into action, is equally important to sustain the momentum. It remains to be seen if our co-created vision for a robust HPSR ecosystem that supports the achievement of SDG 3 could be attained in 5-10 years. The realization of the vision will require co-action among the stakeholders to fulfill their respective commitments. Co-action among the different players in the HPSR ecosystem can enable health systems to deliver quality health services equitably as routine healthcare services and through emergency response, such as during the COVID-19 pandemic. There are no silver bullets to achieve SDG 3, but co-creation with co-action is one potential pathway if we want to turn the disruption from this crisis into a transformative opportunity which, instead of reversing our gains, moves us even closer to achieve healthy lives and wellbeing for all.

Comments