
Dr. Stuart Fischbein, MD, FACOG:
I was trained in an era and a hospital that did not see properly selected breech birth as high risk. I have supported this option my entire 32-year career. In 2010, for reasons having nothing to do with outcomes, my hospital system chose to ban vaginal breech birth as well as vaginal birth after cesarean (VBAC). There was no hearing, no discussion, no review of the literature, and certainly no concern for our ethical obligation to offer reasonable choices to our clients and to allow them the option of informed consent and refusal.
Previously, I had been collaborating with and assisting midwives for three decades as a back-up physician for home birth transports. In 2010, I left the hospital and began my home birth career. Unbound by rigid protocols put in place by committees and risk managers, I was free to individualize my care.
We published this paper to show what can be done with motivated mothers in skilled hands. Success rates of multiparous mothers for vaginal birth in both groups were 100%.
During my years in home birth practice, I became aware that we obstetricians project a lot of anxiety onto the women we care for. In healthy women, pregnancy is a normal physiological bodily function that works best when the women are in a safe, private environment. Midwives are experts at normal birth and, in my experience, their model of care leads to better outcomes and higher rates of satisfaction. We, as obstetricians, can learn much from them. A collaborative model, as I have adopted in our recent study, can lead to better outcomes with less intervention.
Most breech studies compare vaginal breech birth (VBB) to planned cesarean section. We chose to compare VBB to a similar cohort planning vaginal cephalic birth. Selection criteria for breech were more rigid than for cephalic, but outcomes were similar in both groups. Although our numbers were too small to capture rare adverse events, intrapartum transports and perineal integrity were much more related to parity than to presenting part.
While breech birth at home may not be the ideal for most, it remains the only choice for many women in this country other than cesarean for breech birth. We published this paper to show what can be done with motivated mothers in skilled hands. Success rates of multiparous mothers for vaginal birth in both groups were 100%. To not offer VBB to these women is professionally irresponsible. Even primiparous breech mothers had a 76% success rate at home. This information deserves a place in informed consent discussions.
Our efforts should not be put into restricting choice but into honoring our ethical obligations to the women we serve. We can support this goal by learning and then teaching the skills that make our profession unique, by supporting colleagues who offer vaginal breech birth, and by advocating for more robust breech training & education from our professional societies.
Rixa Freeze, PhD:
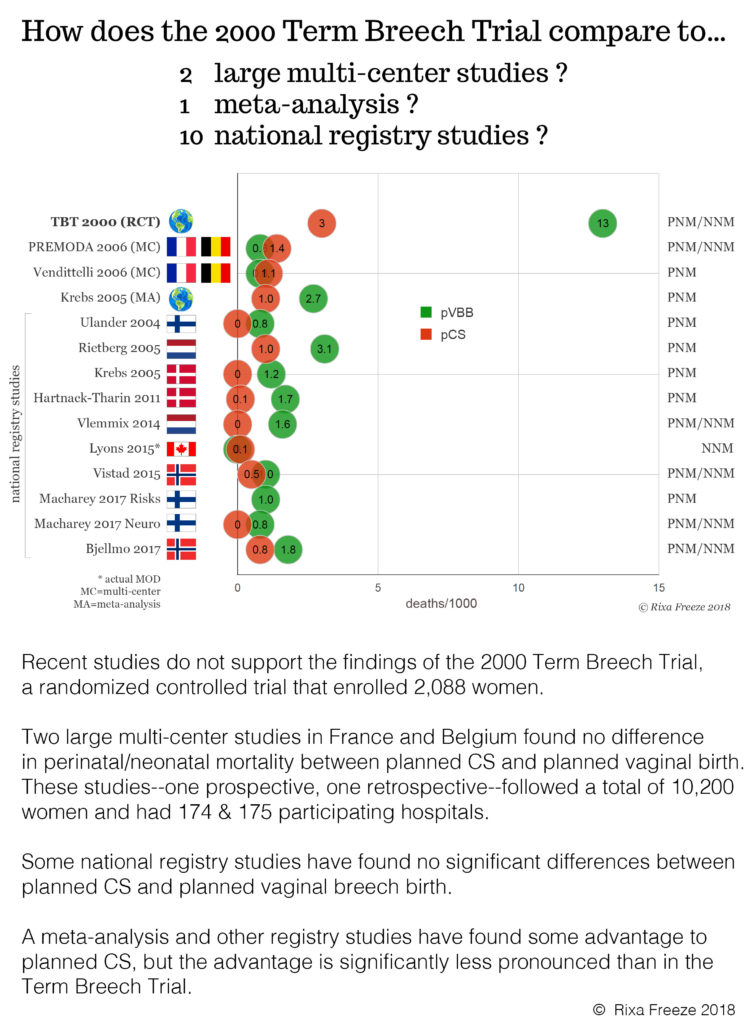
Evidence since the Term Breech Trial is clear that the short-term risks of VBB to the baby are small—sometimes even identical to planned cesarean section (see infographic below).
And we cannot forget the long-term risks of cesarean section to the baby and the short- and long-term risks to the mother. Despite this evidence, VBB is nearly impossible to obtain in the United States. For many women, the only option for a vaginal breech birth is at home.
Our study is the largest of its kind on breech birth at home. Larger datasets exist, but they do not include information about provider skill level, selection criteria, type of breech presentation, or whether the breech presentation was diagnosed before the onset of labor—all factors we addressed in our study.
We found that breech birth at home leads to high rates of vaginal birth and good maternal outcomes (including postpartum transfers, blood loss, and perineal integrity). However, with only 50 breech presentations at the onset of labor, our sample size is too small to draw conclusions about uncommon adverse neonatal outcomes.
We need more high-quality data on home breech outcomes. What if we could analyze 500 home breech births rather than 50?
We are doing women enormous harm by taking away their bodily autonomy when their baby is breech. In theory, state and federal laws support the principle of informed consent and informed refusal, and nearly every hospital has a patient’s bill of rights that ensures consent before medical procedures. Yet we throw these legal and ethical rights away when a baby turns bottom-first.
We can do better. We owe it to the women we care for. Women should not be forced to leave the hospital in order to exercise their right to informed consent. Every woman with a breech baby deserves access to skilled providers in her own community who can support her, whether she chooses a planned cesarean section or a vaginal breech birth.
Comments